|
INTRODUCTION
Althogh hand grip
strength is sufficient for evaluation of results in flexor tendon repair ,the knowledge of finger flexion strength can be
a valuable adjunct in analysing the patient with subjective and/or objective weakness in their hands or fingers.therefore
,for the purpose of monitoring the isolated finger flexor strength ,the newly designed instrument for evaluation of the same
was introduced . Also considering the common incidence of reduced finger flexor strength in the injured finger isolated finger
flexor exerciser with audio-visual feedback was designed, so that the exercise regime for the individual finger can be focused
with the added advantage of audio-visual feedback.
AIMS AND OBJECTIVES
Study has been conducted by keeping in
mind following aims And objectives
1. To introduce the new method of evaluation for assessing the isolated finger
flexor strength.
2. To introduce the instrument for measuring isolated finger flexor strength.
3. To collect
the normative data for isolated finger flexor strength and grip strength.
4. To calculate the ratio of,
a. hand
grip strength,
b. isolated finger flexor strength of index finger ,middle finger ,ring finger & little finger.
Between
dominent & non dominent hand in normal population.
5. To find out the relationship between grip strength and isolated
finger flexor
strength
6. To use the above mentoined ratio for setting up the target for the injured
hand in cases
of flexor tendon repair.
7. To study the effectiveness of the newly and indigenously designed instrument "isolated finger
flexor exerciser with audio-visual feedback" on grip strengthening in cases of primary flexor tendon repair as opposed to
the activities used conveniently in occupational therapy treatment programme.
METHODOLOGY
The study was divided
in two parts:
a. study of normal population
b. study of patient population
Study of normal population
The
study of normal population included 40 subjects, all men, from 15-30 year age group , with right hand dominance. They belonged
to various occupations. Grip strength was tested first and then the isolated finger flexor strength followed by finger length
measurement. Isolated finger flexor strength was evaluated with the help of evaluation instrument specially designed to do
so , as shown in the photograph.
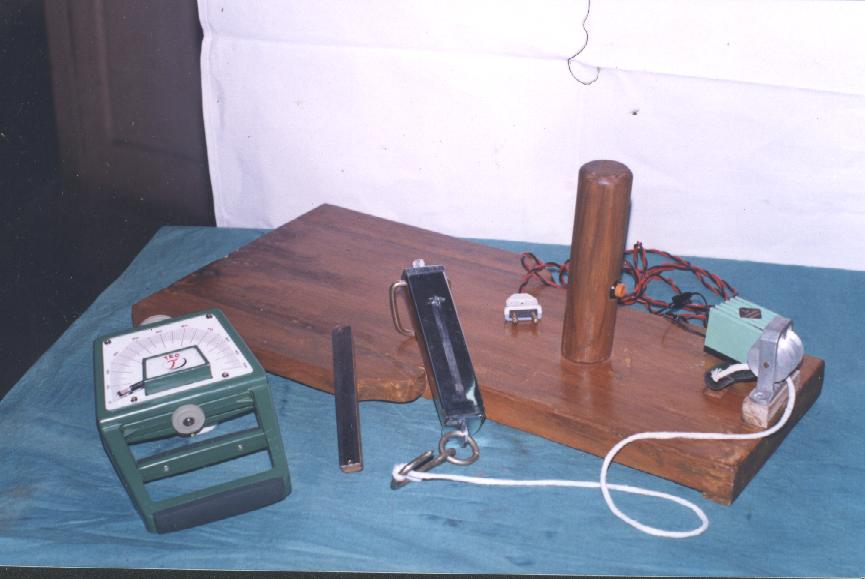
APPARATUS
The basic principle of the method was that, the force in each fingertip
was measured when patient grips a vertical cylinder with maximal strength. The push button was fixed inside the cylinder which
was in turn connected to the buzzer.
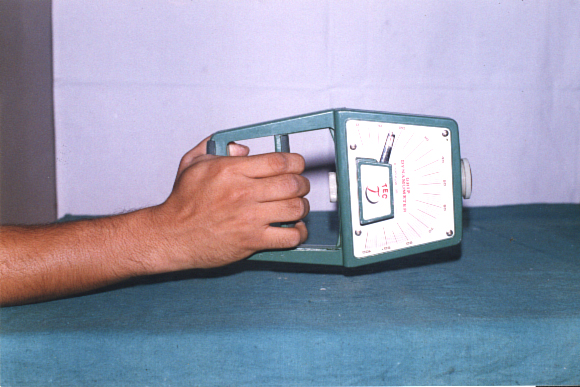
PROCEDURE
The subject was instructed to grip the cylinder with maximal
strength with the position of the finger to be tested on the push button, so that the buzzer sounds. The therapist applied
maximal force within couple of seconds, gradually pulling the spring balance, until the distal phalanx of the finger lost
contact with the cylinder surface. The loss of contact with cylinder surface was indicated by termination of the buzzer sound
& at the same time, the force was noted on the spring balance. This was called as ?lated finger flexor strength??lt;br>Study
of Patient Population The study of patient population included 14 subjects , all males from 16-30 year age group with right
handed dominance.
Patient Selection Criteria
1. Patient with pure flexor tendon injury i.e. without any major
nerve involvement or fracture.
2. Patient with primary flexor tendon repair in any zone .
Patients selected were
from zone II to IV & belonged to various occupations.
ASSESSMENT
All patients were first assessed after
8 weeks of 9 repair & followed by assessment after every week for 4 weeks i.e. upto 12weeks after repair. The patient
population was divided into two groups:
1.Conventional group
2.Experimental group
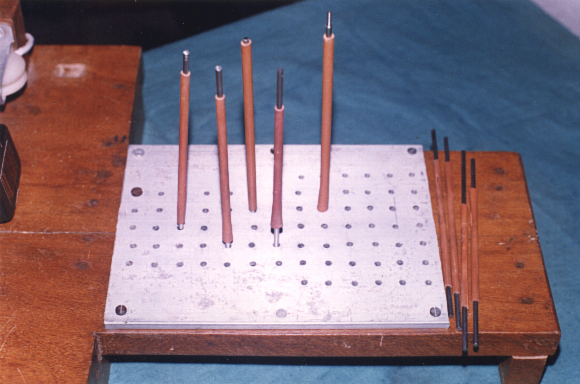
Conventional group
subjects were given following activities, for one-hour daily - foam squeezing, spring loaded gripper, hand gripper, magnetic
peg lifting, karate board.
Experimental Group Subjects from experimental group were given islated finger Flexor Exerciser
with Audio-visual Feedback for half an hour in addition to the above-mentioned activities used in control group which were
also given for half an hour.
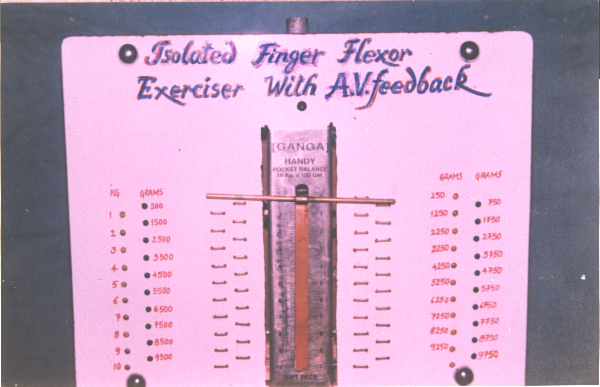
ISOLATED FINGER FLEXOR EXERCISER WITH
AUDIO-VISUAL FEEDBACK
As shown in the
photograph
This particular instrument consist of
- Hand piece and
- Audio visual feedback piece
Hand piece,
in turn consist of two distinct parts,
- Pulley system
- Platform for the placement of the hand for exercise
Audio-visual
feedback piece was also mounted on the wooden plank with the help of iron rod nut and bolts. This piece consist of a spring
balance with minimum calibration of 100 gram and parallel to this was the Audio-visual feedback circuit. Feedback indicator
in the form of light and sound was given after the exercising finger achieves every 250 grams of force. While exercising,
placement of the forearm of the involved hand was in mid-prone position with 15 to 20 degrees of dorsiflexion, with the help
of niwar straps. Depending upon the joint to be moved in the finger i.e. MP, PIP, DIP, the joints were stabilized with the
help of padded stabilizing steel rods.
Both the groups were given similar home programme, which included following activities.
- Cloth clops ,Clay molding,Spring loaded gripper ,Towel squeezing ,Dough making
OBSERVATIONS AND DISCUSSION
The
results of the study reveals that the improvement of grip strength and isolated finger flexion force in the experimental group
was significant
(P < 0.05) and establishes the fact that the newly designed exerciser was an effective means of grip
strengthening, following flexor tendon repair. The findings have also proved that the regime of therapy which was administered
on the experimental group achieved much faster recovery. Thus newly designed instrument proved to be a valuable adjunct to
the conventional activities.
In the study of normal population, the grip strength and isolated finger flexor strength
were greater in the dominant hand. Also the mean force pattern between the four digits showed middle finger being the strongest,
followed by index, ring and little finger in both the hands.However, the grip strength ratio between dominant and non-dominant
hand remained constant the similar relationship was observed for isolated finger flexor strength in respective digits of dominant
and non-dominant hand.
In 1981, Arvid Ejeskar did a methodological study to evaluate isolated finger force. He used dynamometer
to note down the force and attempts were made to observe small finger motion of the DIP joint of the finger in order to overcome
difficulty in observing small finger motion in the DIP joint and simultaneously noting down the reading.This study used a
buzzer signal, so that more accurate reading can be obtained. Thus the newly introduced method allows, measurement of isolated
finger flexor strength in a standardized and accurate manner for power grip. Both the instruments used for measuring strength
had shown higher test-retest reliability. Also face validity and content validity of the newly designed instrument was confirmed.
The mean force pattern between the four digits was similar to that reported by Arvid Ejeskar (1981) i.e. the middle finger
being the strongest, followed by index, ring and little finger in both, the dominant and non-dominant hand.
Thorngren
et al (1979) and Arvid Ejeskar (1981) suggested that, the ratio of dominant and non-dominant hand strength could be a useful
parameter in evaluation of expected recovery under pathological condition. So, in my study also the ratio obtained from the
study of normal population was used to calculate the expected recovery in the injured hand.
Isolated finger flexor strength
improved significantly in experimental group as compared to the conventional group. This may be because of exercise was given
to only one finger at a time. Another reason could be emphasis on exercise given for the muscles acting at each joint at finger
with adequate proximal joint stabilization and third reason could be continuous, instantaneous feedback, which was also directly
proportional to the amount of finger strength. Thus, increase isolated finger flexor strength may have improved the overall
grip strength.
CONCLUSION
After analyzing the data it can be concluded that the newly designed instrument
was an effective means of improving isolated finger flexor strength and in turn grip strength, as seen with the performance
in the experimental group (P < 0.05). Also because of the efficiency of this instrument, the recovery was much faster.
This study also introduced a new instrument of evaluation to measure isolated finger flexor strength and was found to
be reliable (r=0.970) and valid.
Other uses of the newly designed instrument could be,
 Gliding exercises
 Resistive exercises for other conditions where grip strength / isolated finger flexor strength is affected.
Selected strengthening of tendons of the hand as a part of pre and postoperative management of tendon transfer.
Finally,
I would also like to mention that,
 Follow up study is definitely needed.
 Further study with
larger population is needed.
REFERENCES
A. Journals
1. Adolfsson L., Soderberg G, Larsson M, Karlander L.E
(1996) The effect of a shortened postoperative mobilization program after flexor tendon repair in zone II. The Journal of
Hand Surgery 21B: 1: 67-71.
2. Bens E. Doris, Brewer Semyon E ??974) The Hand Gym: An exercise apparatus for patient with
rheumatoid arthritis. Archieves of Physical Medicine and Rehabilitation ?? : 477-480.
3. Ejeskar Arvid, Ortegren R. (1981),
Isolated Finger Flexion Force. A Methodological Study. The Hand ??: 3 : 22.
4. Ejeskar Arvid (1987), Finger flexion force
and hand grip strength after tendon repair, The Journal of Hand Surgery, 7: 1 : 61.
5. Johnston Mark V. Keith Robert Allen,
Hinderer Steven R. (1992). Measurement standards for interdisciplinary medical rehabilitation. Archives of Physical Medicine
and Rehabilitation ??: 12-5 : 53-523.
6. Kulkulka C. G., Brown Mike, Basmajian J.V. (1975) Biofeedback training ??r early
finger joint ??bilization. American Journal of Occupational Therapy ??: 469-470.
7. Kumar J.P. (1992) The handy exerciser.
The American journal of Occupational Therapy 46: 8: 762-764.
8. Mathiowetz Virgil, Kashman Nanaj, Vallan Gloria, Weber
Karen, Dowe Mary. Rogers Sandra (1985). Grip and pinch strength: Normative data for adults. Archieves of physical medicine
and Rehabilitation 66: 69-74.
9. Spector Paulu Frierson Ada (1976), Modified finger exercise board ??e American Journal
of Occupational Therapy ??: 6 : 380-383.
10. Thorngen K.G., Werner C. O. (1979) Normal grip strength. Acta Orthopaedica
Scandinarica ??: 255-259.
11. Rehabilitation of Hand ??d Edition (1990), Hunter, Schneider, Callahan, Mackin, The C. V.
Mosby Company.
ACKNOWLEDGEMENT
If you would not be forgotten,
as soon as you are dead and rotten.
either
write things worth reading,
or do things worth the writing
Benjamin Franklin
Words have their own handicaps. At
no time is this more apparent than when one tries to put in words his feeling of gratitude for those who have helped in a
trying venture. This work nevertheless, shall be incomplete, if I don?ut or record my heart felt gratitude.
It is my proud
to express my sincere regards, deep sense of gratitude to my guides Mr. S.B.A. Sams and Mrs. Sheela Rao for their invaluable
and most needed guidance and co-operation during the period of my dissertation.
I would also like to convey my sincere
thanks to Mrs. I.R. Kenkre, Head of Department, Occupational Therapy Department and Mrs. P.M. Pai, Dean K.E.M. Hospital, for
allowing me to conduct this study in the institute.
I am also thankful to Mrs. R.E. Rana, Head of Department, Plastic
Surgery, K.E.M. Hospital for referring me patients from her unit.
I also express my sincere gratitude to Mr. Kailash Gandewar
for guiding me regarding statistics of the study.
Last but not the least, I give a million thanks to my subjects of flexor
tendon repair.
Dr. Hemant P. Nandgaonkar
  |